Single-Cell Perspective: Deciphering Key Immune Cells for NSCLC Brain Metastasis ICI Response
I. Research Background
Brain metastasis (BrM) is one of the most severe complications of advanced non-small cell lung cancer (NSCLC), with extremely poor prognosis and short median survival. With continuous improvements in NSCLC diagnosis and treatment, patient survival has been prolonged, and the incidence of brain metastasis has also increased year by year, becoming a key factor limiting patient quality of life. The advent of immune checkpoint inhibitors (ICIs) has brought new therapeutic hope to patients with NSCLC brain metastases. However, clinical practice has revealed significant heterogeneity in ICI efficacy in this population, with intracranial objective control rates ranging only from 16.4%-52.5%. Only a minority of patients achieve complete response, while the majority cannot benefit. Due to the inherent heterogeneity of brain metastases, their genomic and transcriptomic characteristics differ significantly from extracranial tumors. Extracranial tumor biomarkers are ineffective in predicting intracranial response to ICIs, and brain metastasis biopsy carries high surgical risks and technical difficulties, limiting clinical application. Cerebrospinal fluid (CSF), as a minimally invasive liquid biopsy sample, can accurately reflect the immune status of the brain metastasis microenvironment and has become an ideal vehicle for assessing intracranial immune responses. Based on this, Li Y-S and colleagues published a study in Journal for ImmunoTherapy of Cancer to explore the key immune cell subsets associated with ICI response in NSCLC brain metastases through single-cell sequencing of CSF and brain metastasis tissues.
II. Research Methods
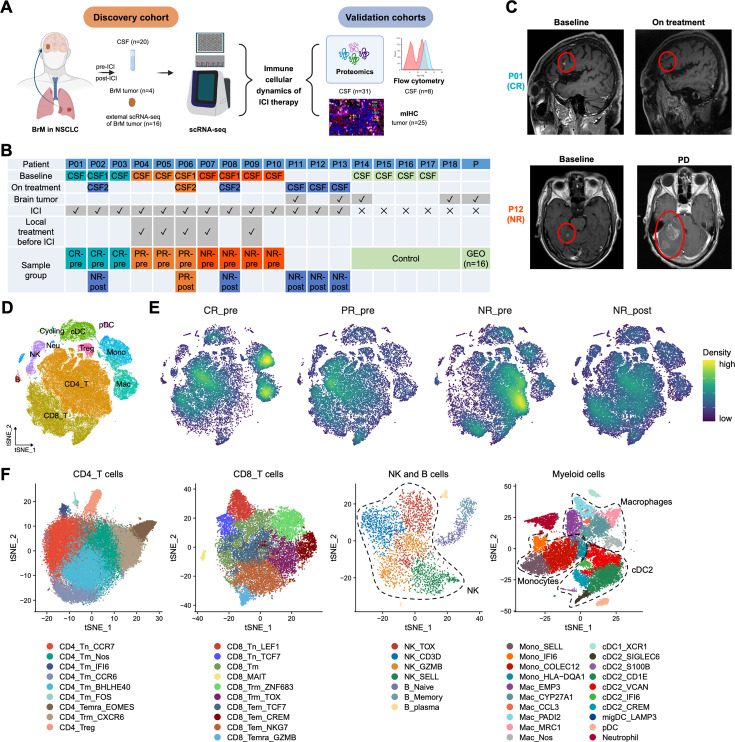
This study employed a rigorous multi-technology, multi-cohort research design, prospectively enrolling NSCLC brain metastasis patients planned to receive ICI treatment. Core datasets included CSF samples from 20 patients before and during ICI treatment, brain metastasis tissue samples from 4 patients, and single-cell RNA sequencing (scRNA-seq) data from 16 brain metastasis samples from public databases (GEO). To ensure reliability and reproducibility, 31 CSF samples were collected for proteomic analysis, 25 brain metastasis tissue samples for multi-color immunohistochemistry (mIHC/IF) validation, and 8 CSF samples for flow cytometry validation, forming a multi-dimensional validation system.
The study used scRNA-seq technology to perform single-cell transcriptomic analysis on CSF and brain metastasis samples. After quality control, data normalization, batch effect removal, dimensionality reduction, and unsupervised clustering, immune cell subsets were identified using known cell marker genes. Cell developmental trajectories and state transitions were analyzed using PAGA, RNA velocity, and other methods. CellChat software was used to predict intercellular communication relationships. AUCell, GSEA, and other analytical tools were employed to evaluate cell function and pathway activity. Flow cytometry was used to validate the presence and functional characteristics of key immune cell subsets. mIHC/IF was used to detect the abundance of key cell subsets in brain metastases. Proteomic analysis validated the activation status of key pathways. Multiple public datasets were integrated to further extend the generalizability of the findings. Samples were grouped based on ICI treatment status and efficacy: confirmed responders (CR, achieving effective response without brain radiotherapy), potential responders (PR, requiring combination with brain radiotherapy for effective response), non-responders (NR, no response or disease progression after treatment), with untreated samples as controls. Inter-group comparative analysis identified key immune features associated with intracranial ICI response.
III. Results Analysis
1. Single-Cell Profiling of NSCLC BrM Under ICI Treatment
The study performed scRNA-seq analysis on collected CSF and brain metastasis samples, retaining transcriptomic data from 100,051 high-quality single cells for subsequent analysis. 11 major immune cell types were successfully identified, including CD4+ T cells, CD8+ T cells, B cells, natural killer cells, etc., constructing a detailed immune cell atlas integrated with ICI treatment information. t-SNE visualization clearly presented the distribution characteristics of all immune cells, intuitively demonstrating the diversity of immune cells in CSF, with CD4+ T cells being the most abundant immune cell type in CSF. Grouped scatter plots showed that the CR group had significantly more macrophages before treatment, and the proportion of CD4+ T cells in the CR group increased after treatment, indicating dynamic changes in the immune microenvironment during ICI treatment.
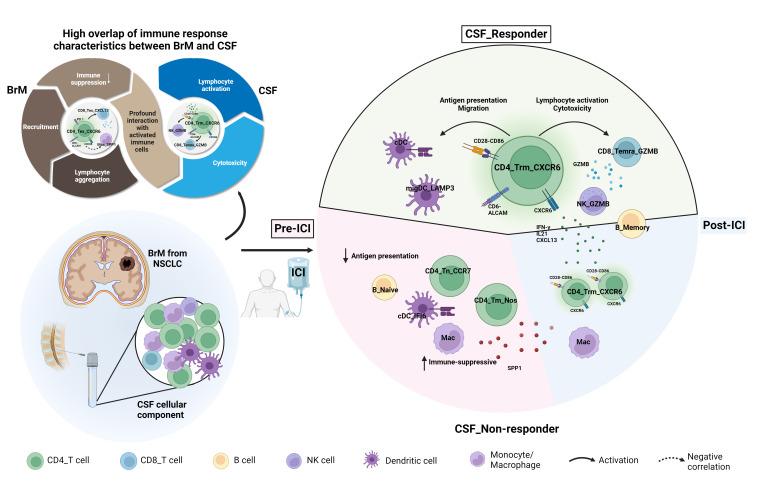
2. CD4_Trm_CXCR6 Cells Are Key Subsets Associated with Intracranial ICI Response
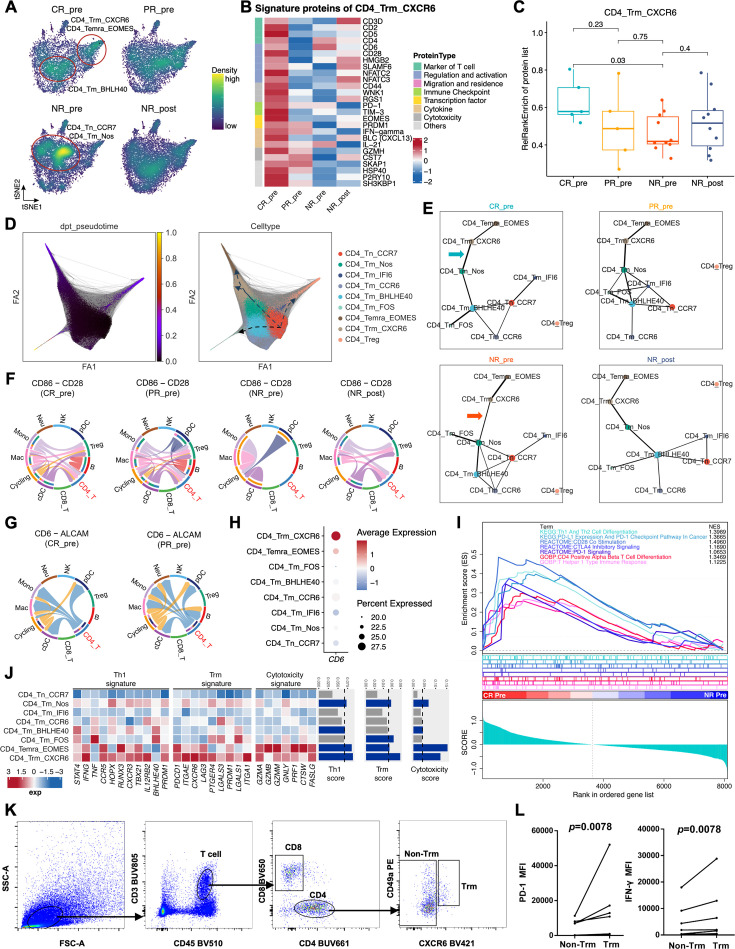
As core regulatory cells of the immune system, CD4+ T cell subsets and functional states are closely related to ICI response. The study further divided them into 9 subsets. Inter-group comparison revealed that in non-responder patients before ICI treatment (NR-pre), CD4+ T cells mainly consisted of naive T cells (CD4_Tn_CCR7) and memory T cells, while in the CR group before treatment, CD4_Trm_CXCR6 cells were significantly enriched. These cells highly expressed CXCR6, PDCD1, and other markers, showing characteristics of tissue-resident memory T cells. Pseudotime trajectory analysis showed that CD4_Trm_CXCR6 cells were in a late differentiation state and were significantly expanded in the CR group, suggesting their important role in ICI response.
Proteomic validation results showed that in CSF before CR treatment, characteristic proteins of CD4_Trm_CXCR6 cells (such as CXCL13, TIM-3) were highly expressed. Heatmaps clearly showed protein expression differences between groups. The study used a custom relative rank enrichment algorithm to score characteristic proteins and estimate cell abundance. Results indicated that CD4_Trm_CXCR6 cell abundance before treatment in the CR group was significantly higher than in NR group, with statistically significant differences. PAGA analysis revealed the developmental relationship between CD4+ T cell subsets, with CD4_Trm_CXCR6 cells representing a terminal differentiation state associated with ICI response.
Cell-cell communication analysis showed that overall immune cell interactions and CD4+ T cell-specific communication strength in the CR group were significantly higher than in the NR group. Among them, the CD86-CD28 co-stimulatory signal was significantly enriched before treatment in the CR group, potential responder group (PR), and after treatment in the NR group, suggesting its important role in immune activation. Further analysis showed that CD4_Trm_CXCR6 cells mainly received signals from antigen-presenting cells (APCs) and sent signals to CD8+ T cells, indicating their regulatory role in the immune response network.
3. Functional Consistency of CD4+PDCD1+CXCR6+ T Cells in CSF and Brain Metastasis Patients
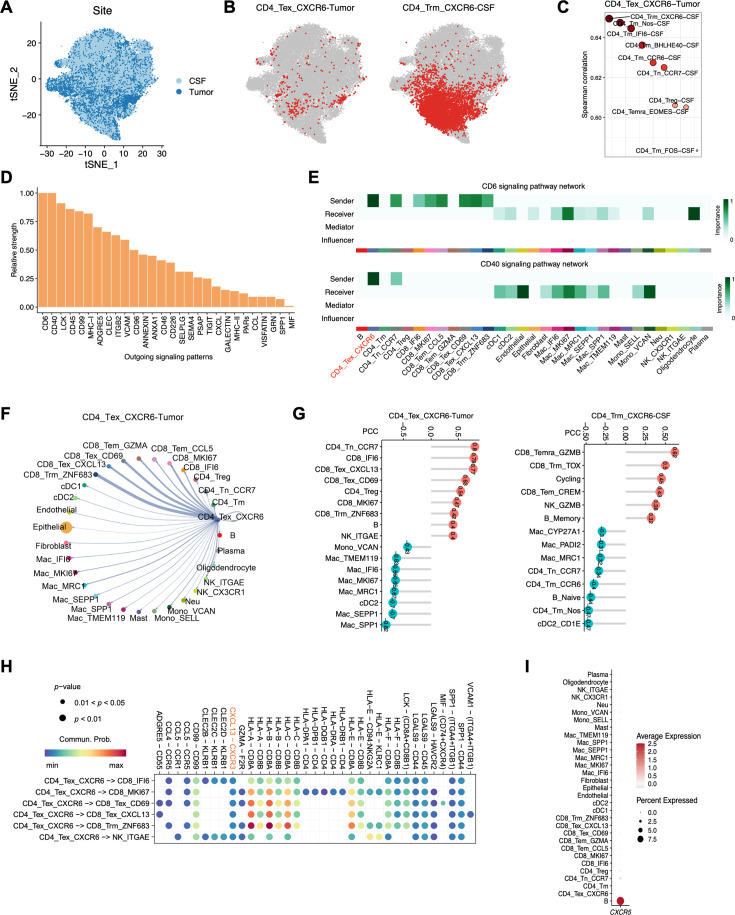
The study further integrated scRNA-seq data from 20 NSCLC brain metastases to explore ICI response-related exhausted T cell (Tex) subsets in brain metastases. Three Tex cell subsets were identified. Among them, CD4_Tex_CXCR6 cells in brain metastases and CD4_Trm_CXCR6 cells in CSF had highly similar transcriptomic characteristics, both highly expressing PDCD1, CXCR6, and other markers, suggesting they may represent the same cell population with different tissue localization.
Scatter plots merging CSF and brain metastasis CD4+ T cells showed high overlap in the dimensionality reduction space. Dot plot quantitative analysis further confirmed that CD4_Tex_CXCR6 cells were highly correlated in gene expression profile with CD4_Trm_CXCR6 cells in CSF, providing important evidence for CSF as a surrogate sample for the immune microenvironment of brain metastases. Functional analysis showed that the strongest outgoing signal of CD4_Tex_CXCR6 cells was mediated by CD6, which was completely consistent with the signal characteristics of CD4_Trm_CXCR6 cells in CSF. CD40 signal was significantly enriched in CSF CD4+ T cells before CR treatment, suggesting its role in activating anti-tumor immune responses.
Cell abundance correlation analysis showed that the abundance of this cell subset was positively correlated with activated lymphocytes (such as CD8+ T cells, B cells) and negatively correlated with immature lymphocytes and immunosuppressive myeloid cells. Ligand-receptor interaction analysis showed that it could recruit activated immune cells by secreting CXCL13, and only this cell subset in brain metastases expressed the anti-tumor cytokine IL-21. Together, these findings confirm its key role in connecting the immune microenvironment of CSF and brain metastases and regulating anti-tumor immune responses. They can be collectively defined as CD4+PDCD1+CXCR6+ T cells.
4. Predictive Value and Distribution Characteristics of CD4+PDCD1+CXCR6+ T Cells
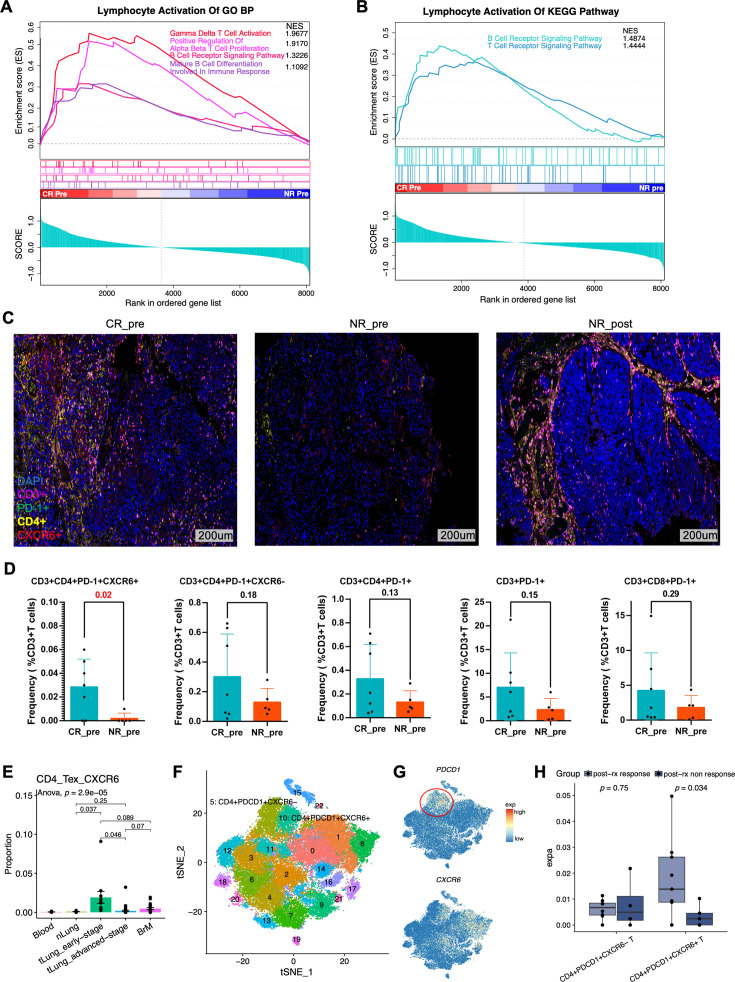
To verify the clinical predictive value of CD4+PDCD1+CXCR6+ T cells, the study detected the abundance of this cell subset in brain metastasis tissues using mIHC/IF. Results showed that the number of CD4+PDCD1+CXCR6+ T cells in brain metastases before treatment in the CR group was significantly higher than in the NR group, while other PD-1 positive cell subsets (such as CD4+PDCD1+CXCR6-, CD8+PDCD1+) showed no significant differences between groups, confirming its specificity as a predictive marker for intracranial ICI response. Representative mIHC staining images and bar charts intuitively presented the enrichment characteristics and inter-group differences of this cell subset in different responder groups, further supporting its predictive value.
Integrated analysis of multiple public datasets found that CD4+PDCD1+CXCR6+ T cells are almost absent in peripheral blood, relatively rare in normal lung tissue, but significantly enriched in primary lung cancer tissue and brain metastases, showing obvious tumor specificity. This explains why peripheral blood biomarkers are difficult to predict intracranial ICI response. Further analysis showed that CD4+PDCD1+ T cells can be clearly divided into CXCR6+ and CXCR6- subsets. The CXCR6+ subset highly expresses cytotoxicity-related genes such as IFNG and PRF1, and ICI treatment can further enhance its activation status, suggesting its potential role in anti-tumor immunity.
5. Synergistic Mechanism Between Dendritic Cells and CD4+PDCD1+CXCR6+ T Cells
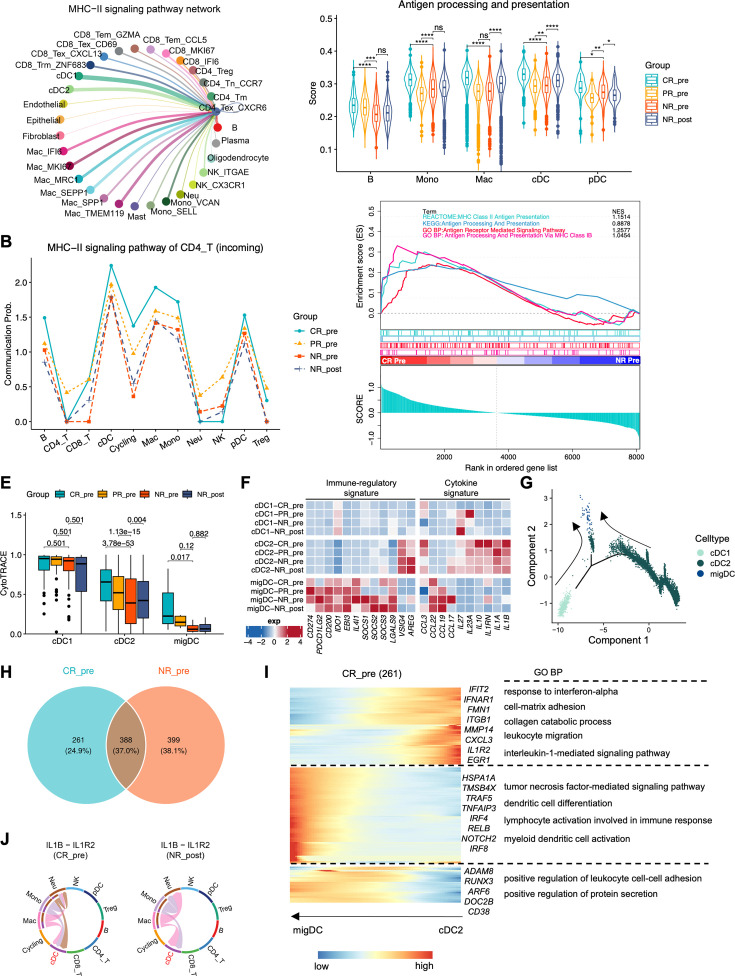
Antigen-presenting cells (APCs) play a key role in activating T cell immune responses. The study found that the strongest signal received by CD4_Tex_CXCR6 cells comes from the MHC-II pathway, with cDCs, monocytes, and other APCs being the main sources of this signal. Network visualization clearly presented the close communication between APCs and CD4_Tex_CXCR6 cells. Further analysis showed that CD4+ T cells in CR group CSF received significantly stronger signals from APCs (especially cDCs) than NR group, indicating more effective antigen presentation in the responder group.
Functional analysis showed that APCs before treatment in the CR group had higher antigen processing and presentation function scores. Proteomic analysis also confirmed that proteins related to MHC-II-mediated antigen presentation were significantly enriched in CSF before CR treatment. CSF cDCs were mainly divided into three subsets: cDC1, cDC2, and migDC. CytoTRACE analysis showed that cDC2 had stronger proliferative capacity and developmental potential in the CR group, which may be related to its ability to better activate T cell responses.
Developmental trajectory analysis of cDCs showed that cDC2 can differentiate into migDC. In the CR group, this differentiation process enriches inflammation and immune activation-related genes, which can promote immune response initiation. In contrast, the NR group differentiation process enriches immune-unrelated genes and cannot effectively activate T cells. In addition, the IL1B-IL1R2 inflammatory signaling pathway was only significantly enriched in the CR group, further supporting the active pro-inflammatory microenvironment in responder CSF, providing favorable conditions for ICI response.
6. Pro-Inflammatory Activation Characteristics of Responder CSF and Role of Monocyte Subsets
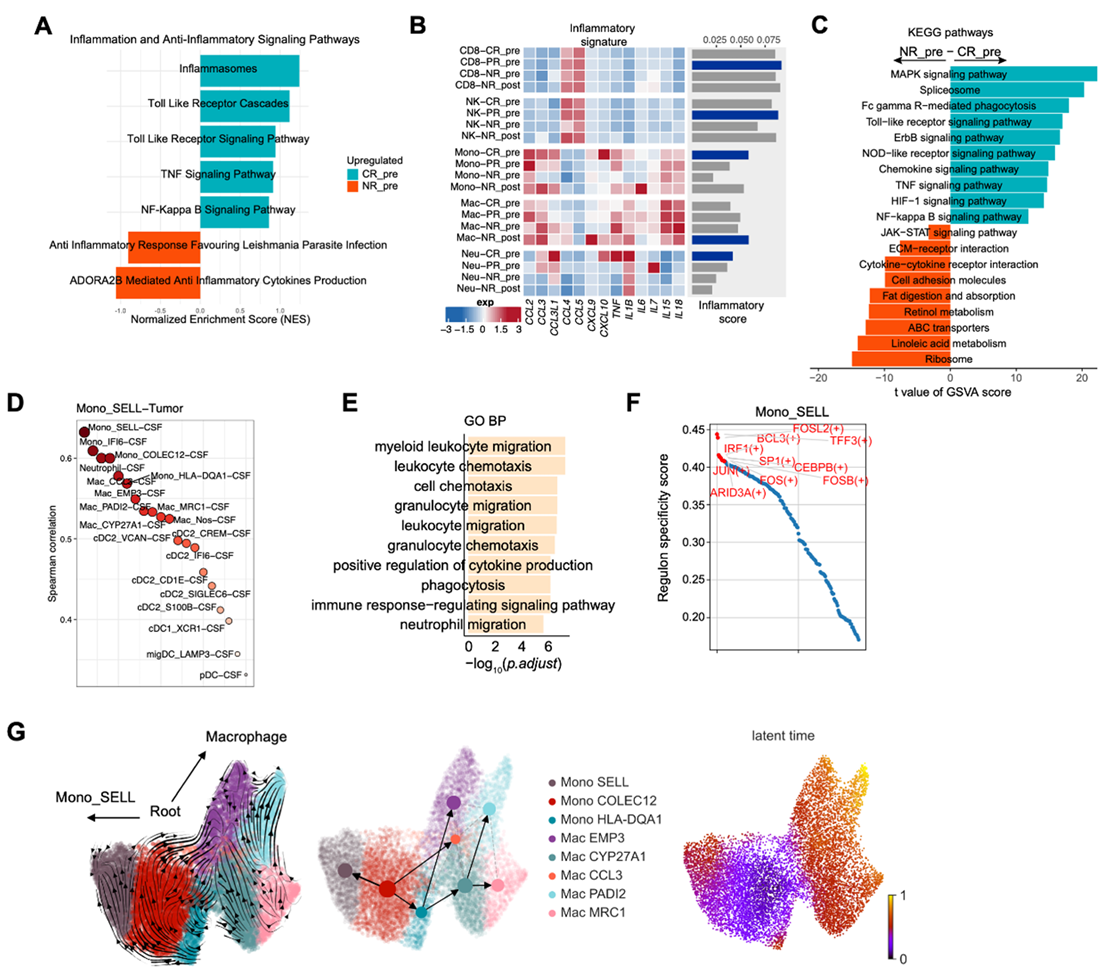
Proteomic pathway enrichment analysis showed that pro-inflammatory pathways such as tumor necrosis factor and NF-κB were significantly enriched in CSF before CR treatment, suggesting that the cellular microenvironment is in an active pro-inflammatory state, which can effectively promote immune cell activation and enhance ICI treatment efficacy. Monocytes in responder CSF have higher inflammatory activity. The Mono_SELL subset was significantly enriched before CR treatment and after NR treatment. This subset highly expresses genes related to immunotherapy response such as SELL and CFP. Previous studies have confirmed that such monocytes can serve as predictive factors for immunotherapy response in primary NSCLC patients, and this study further extends their clinical significance.
Developmental trajectory analysis of monocyte-macrophage showed that Mono_COLEC12 is the differentiation starting point of monocytes, which can differentiate into Mono_SELL cells and macrophages, suggesting that Mono_SELL represents a differentiation direction independent of macrophages and is closely related to ICI response. Mono_SELL cells enrich genes related to migration, chemotaxis, and cytokine production, can recruit and activate other immune cells, and have high activity of activator protein 1-related transcription factor networks, which can regulate immune cell activation and cytokine secretion, further participating in pro-inflammatory responses and immune activation.
IV. Conclusions and Prospects
Using multiple technical approaches including scRNA-seq, proteomics, and mIHC/IF, combined with multi-cohort validation and public dataset integration, this study systematically mapped the immune cell landscape of CSF and brain metastases before and after ICI treatment in NSCLC brain metastasis patients, identifying CD4+PDCD1+CXCR6+ T cells as key predictors of intracranial ICI response. This cell subset is significantly enriched in both CSF and brain metastases before treatment in responder groups, with highly similar transcriptomic and functional characteristics. It can synergize with cDCs to promote anti-tumor immune responses through mechanisms such as activating co-stimulatory signals and recruiting activated immune cells. An active pro-inflammatory microenvironment exists in responder CSF, and the Mono_SELL monocyte subset can serve as a complementary marker for ICI response prediction.
The clinical significance of this study is significant: On one hand, CD4+PDCD1+CXCR6+ T cells in CSF can serve as a minimally invasive and reliable biomarker for screening NSCLC brain metastasis patients who benefit from ICI treatment, avoiding adverse reactions and medical resource waste caused by ineffective treatment, and providing guidance for clinical precision treatment. On the other hand, this cell subset and its related signaling pathways such as CD6-ALCAM and MHC-II, as well as the Mono_SELL monocyte subset, can serve as potential therapeutic targets, providing new directions for optimizing ICI combination treatment strategies, which is expected to further improve ICI efficacy in NSCLC brain metastasis patients.
At the same time, this study has certain limitations. For example, the sample size for scRNA-seq analysis is limited, and future large-scale prospective studies are needed to further validate the conclusions. In addition, the migration patterns of T lymphocytes between brain tissue, CSF, and peripheral immune system during ICI treatment, as well as the specific regulatory mechanisms of CD4+PDCD1+CXCR6+ T cells, still need further investigation. Future research can further improve the ICI response prediction system, providing more solid theoretical support and practical guidance for precision immunotherapy in NSCLC brain metastasis patients.
References
Li YS, Lai W, Yin K, Tu HY, Li L, Lin SH, Li P, Zhou DX, Guo WB, Yang JJ, Zhou Q, Zhong WZ, Zhang XC, Jiang BY, Wang Z, Yang XN, Wang BC, Pan Y, Chen HJ, Xu CR, Zeng L, Chen ZH, Yan HH, Sun H, Dong ZY, Liu SM, Li Y, Luo OJ, Zheng MM, Wu YL. Cellular dynamics in cerebrospinal fluid unveils the key regulators of intracranial response to immune checkpoint inhibitors in NSCLC brain metastases. J Immunother Cancer. 2025 Nov 28;13(11):e012071. doi: 10.1136/jitc-2025-012071. PMID: 41314983; PMCID: PMC12666088.