Literature Sharing: Multiplex Immunofluorescence Study Reveals PD1-Negative Regulatory T Cells as Prognostic Markers for Chemotherapy in Colorectal Cancer
1. Research Background
Among global malignant tumors, colorectal cancer (CRC) has become one of the core tumor diseases threatening human health due to its extremely high morbidity and mortality. Stage III CRC, as a critical phase of locally advanced disease, is the main target for clinical postoperative adjuvant chemotherapy and also a challenge in prognostic stratification. Currently, the standard treatment for stage III CRC patients is the FOLFOX chemotherapy regimen combining oxaliplatin with fluoropyrimidines. However, extensive clinical data shows that the benefit population of this treatment is extremely limited — less than 20% of patients can achieve disease control through postoperative adjuvant chemotherapy, while over half will develop distant metastasis and disease recurrence. Meanwhile, most non-benefiting patients have to endure long-term toxic side effects of chemotherapy. Currently, clinical practice mainly relies on the AJCC/UICC TNM anatomical staging system to formulate postoperative treatment plans for CRC, lacking precise molecular and immune prognostic biomarkers. It is impossible to effectively distinguish high-risk and low-risk populations for chemotherapy benefits, making individualized precision treatment difficult to achieve. With the deepening of tumor microenvironment research, tumor-infiltrating T lymphocytes have been confirmed as key factors regulating CRC development and affecting patient prognosis. Immune indicators such as immune score and T cell subset infiltration characteristics have gradually become new directions for tumor prognosis assessment. However, previous studies mostly relied on single immune marker detection, failing to accurately distinguish T cell subsets with different functions and truly reflect the immune status of the tumor microenvironment. Based on this clinical pain point, Xanthi Stachtea and other scholars, in the article "Stratification of chemotherapy-treated stage III colorectal cancer patients using multiplexed imaging and single-cell analysis of T-cell populations", innovatively relied on multiplex immunofluorescence imaging and single-cell analysis technology to compare the clinical value of single-marker versus multi-marker combined detection, exploring immune signature models that can accurately predict the prognosis of stage III CRC patients receiving FOLFOX chemotherapy. The aim is to address the shortcomings of existing prognostic assessment systems and provide new technical support and theoretical basis for individualized chemotherapy stratification in CRC.
2. Research Methods
This study adopted a retrospective design. First, 117 stage III CRC patients who received FOLFOX adjuvant chemotherapy were selected as the training cohort, and 191 stage III patients with the same treatment regimen were included to construct an independent validation cohort. All patients did not receive immune checkpoint inhibitor treatment and strictly followed unified inclusion and exclusion criteria to avoid confounding factors such as poor tissue sample quality, insufficient follow-up time, and positive surgical margins. The study relied on multiplex immunofluorescence technology to standardize patient tumor tissue microarrays. Through multiplex staining, imaging, and background correction of immune markers including CD45, CD3, CD4, CD8, FOXP3, PD1, as well as tumor segmentation markers such as DAPI and broad-spectrum cytokeratin, precise single-cell segmentation and localization of the epithelial and stromal regions of tumor tissues were completed. The study also combined pathologist manual scoring and machine learning probability classification algorithms to conduct high, medium, and low-level qualitative assessment and quantitative analysis of immune cell and stromal cell infiltration levels in tumor tissues, accurately dividing eight major T cell subsets including helper T cells, cytotoxic T cells, and regulatory T cells, and distinguishing PD1-positive and negative functional subtypes. On this basis, the study used univariate and multivariate Cox proportional hazards regression models to adjust for clinical confounding factors such as age, tumor stage, and lymph node metastasis, combined with statistical methods including Kaplan-Meier survival analysis, Spearman correlation analysis, and hierarchical clustering analysis, to systematically compare the predictive value of single-marker detection versus multi-marker combined typing on patient disease-free survival and overall survival. Meanwhile, innovative immune hotspot region analysis was conducted to exclude the interference of tumor heterogeneity on experimental results. Finally, the reliability and generalizability of core research conclusions were verified through the independent validation cohort. All statistical analyses were completed using R language, strictly following clinical statistical testing standards.
3. Research Results Analysis
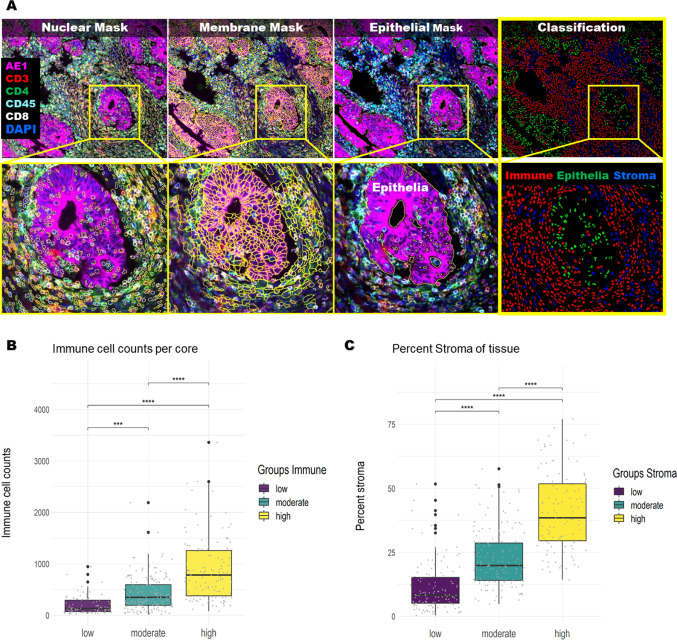
3.1 Consistency Verification Between Automated Detection Technology and Pathological Manual Assessment
Tumor heterogeneity is a core confounding factor difficult to avoid in CRC research. This study first verified the clinical feasibility of multiplex imaging automated detection technology through large-scale tissue samples, laying a technical foundation for subsequent quantitative analysis of immune indicators. The study conducted regional detection on all patients' tumor tissue microarray samples. The results showed that the majority of patients had significant differences in immune cell and stromal cell infiltration among different tissue microarray samples, and over 60% of patients had intratumoral immune heterogeneity. This fully confirmed the spatial heterogeneity of the CRC tumor microenvironment and highlighted the limitations of traditional single-sampling detection. The automated scoring system constructed based on the Cell DIVE platform can accurately quantify immune cell density and stromal cell proportion in tumor tissues. After matching and analyzing the immune scores and stromal scores obtained from automated detection with pathologists' manual three-level scoring results, the two types of assessment results showed extremely strong statistical correlation. Both immune cell infiltration levels and stromal component proportions showed high agreement between automated quantitative data and manual qualitative assessment, with statistically significant differences. This result vividly confirmed the reliability of multiplex immunofluorescence imaging combined with machine learning algorithms. This technology can replace traditional manual slide reading, achieving standardized, precise, and quantifiable assessment of the tumor immune microenvironment, avoiding subjective errors in manual scoring, and breaking through the technical bottleneck that traditional pathological detection cannot achieve single-cell level subtyping and quantitative analysis, providing reliable technical support for subsequent prognostic value mining of T cell subsets.
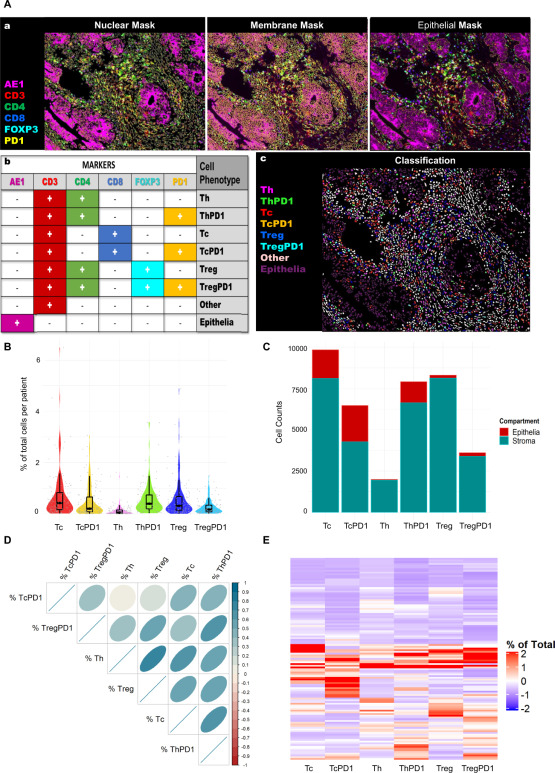
3.2 Multi-Marker T Cell Subset Typing and Tumor Microenvironment Distribution Characteristics
Relying on the technical advantage of simultaneous detection of multiple markers, the study broke through the limitation that single markers cannot distinguish T cell functional subtypes, accurately dividing eight major T cell subtypes and clearly outlining the T cell infiltration panorama of the tumor microenvironment in stage III CRC chemotherapy patients. Through quantitative statistics and spatial localization analysis of all patients' T cell subsets, it was found that cytotoxic T cells and their PD1-positive subtypes were the most abundant T cell subsets infiltrating the tumor epithelial region, while all T cell subtypes were mainly enriched in the tumor stromal region, with overall low immune cell infiltration levels in the epithelial region. This spatial distribution characteristic intuitively revealed that the CRC tumor stroma is the core site where immune cells exert their functions, and also explained the key regulatory role of the tumor stromal microenvironment in tumor immune escape and disease progression. Correlation analysis results showed that the vast majority of T cell subtypes were positively correlated, with only PD1-positive cytotoxic T cells showing extremely weak correlation with helper T cells and regulatory T cells, reflecting that different T cell subsets have differentiated activation and regulatory mechanisms in the tumor microenvironment. After grouping patients' immune landscapes through hierarchical clustering, nearly half of the patients belonged to the low immune infiltration "cold tumor" phenotype, while the remaining patients showed varying degrees of immune infiltration characteristics. Only patients with high immune infiltration "hot tumors" showed better survival trends. Although not reaching statistical significance, this initially confirmed a potential association between overall T cell infiltration levels and patient prognosis, and also provided important clues for subsequent precise screening of prognosis-related specific T cell subtypes.
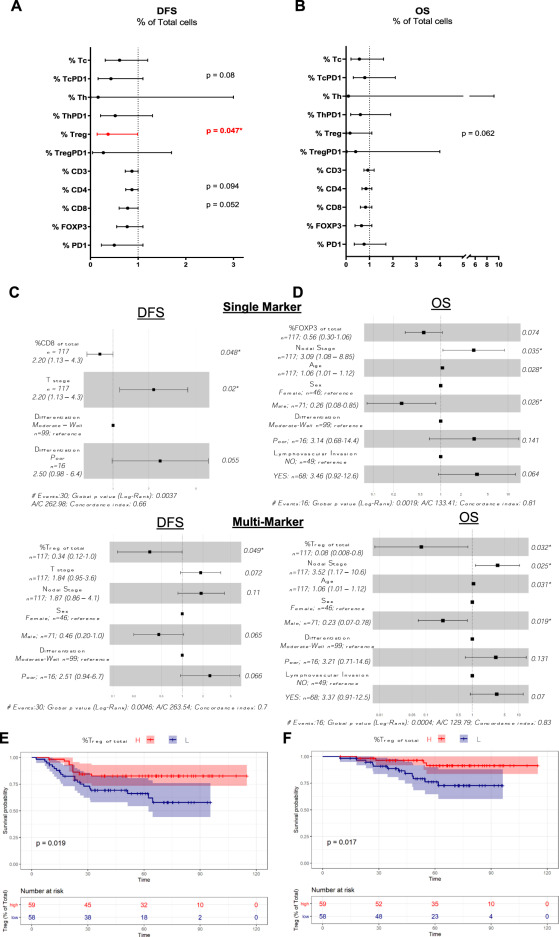
3.3 Predictive Value of T Cell Subset Typing for Patient Chemotherapy Prognosis
The core breakthrough results of this study focused on the correlation analysis between T cell subtypes and chemotherapy patient prognosis, completely overturning the inherent cognition of traditional single FOXP3 marker assessment of regulatory T cell prognostic value, and accurately identifying specific immune markers that can predict the prognosis of FOLFOX chemotherapy patients. Through univariate and multivariate Cox regression analysis, the study found that the expression levels of single immune markers including CD3, CD4, CD8, FOXP3, and PD1 were all unable to effectively predict the disease-free survival and overall survival of stage III CRC chemotherapy patients. Single-marker detection has significant clinical limitations, failing to distinguish immune cells in different functional states and truly reflect the prognostic value of the tumor immune microenvironment. In contrast, PD1-negative regulatory T cells (CD3+/CD4+/FOXP3+/PD1−) defined by multi-marker combination showed strong prognostic predictive ability. After adjusting for all clinical confounding factors including tumor T stage, N stage, differentiation degree, and lymphovascular invasion, patients with high expression of this cell subtype had significantly reduced disease recurrence risk and death risk, with significantly prolonged disease-free survival and overall survival, and the survival differences had clear statistical significance. The corresponding Kaplan-Meier survival curves clearly showed the prognostic stratification trend between high and low expression populations, with patients with high PD1-negative regulatory T cell infiltration showing significantly better long-term survival than those with low infiltration. More importantly, this core conclusion was effectively replicated in the independent FOLFOX chemotherapy validation cohort, with patients with high PD1-negative regulatory T cell infiltration showing significantly improved overall survival, while PD1-positive regulatory T cells had no association with patient prognosis. This fully demonstrates that the prognostic value of regulatory T cells completely depends on their PD1 expression status, and regulatory T cells with different phenotypes play completely differentiated regulatory roles in the tumor microenvironment, explaining the core reason for the controversial association between regulatory T cells and CRC prognosis in previous studies.
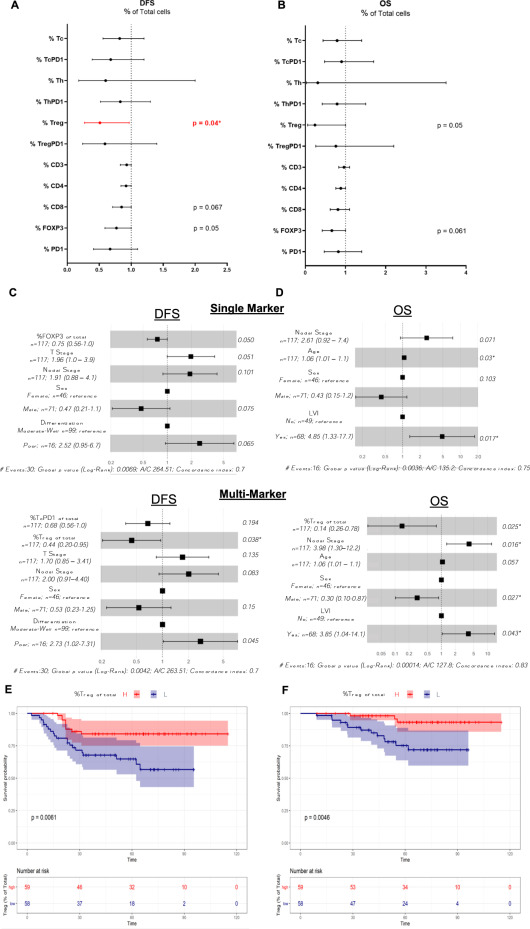
3.4 Prognostic Value Analysis of T Cell Infiltration in Tumor Immune Hotspot Regions
To further exclude the interference of tumor heterogeneity on research results and explore the clinical significance of local high-intensity immune infiltration in tumors, the study innovatively selected the immune hotspot region with the highest T cell density in each patient's tumor tissue for special analysis, improving the limitations of overall average infiltration level analysis. The statistical analysis results of hotspot regions were highly consistent with the overall cohort analysis conclusions, re-verifying that single immune markers have no prognostic predictive value, while high infiltration of PD1-negative regulatory T cells can significantly improve patient disease-free survival, and has marginally significant protective effect on overall survival. Multivariate regression model results further consolidated the core conclusion: in immune hotspot regions, PD1-negative regulatory T cells remained an independent favorable prognostic factor, and their high expression can effectively reduce patient tumor recurrence and death risk, while all other T cell subtypes had no independent prognostic predictive value. This result confirmed the reliability of core immune markers from the perspective of the local tumor microenvironment, indicating that even if there is immune infiltration heterogeneity in the entire tumor, local high-intensity PD1-negative regulatory T cell infiltration can still effectively reshape the tumor immune microenvironment and enhance the anti-tumor effect of FOLFOX chemotherapy, providing more refined reference basis for clinical precise assessment of patient prognosis and formulation of individualized treatment plans.
4. Research Conclusions and Discussion
Through multiplex immunofluorescence single-cell imaging and multi-dimensional statistical analysis, this study systematically confirmed the significant clinical advantages of multi-marker combined T cell typing compared with traditional single-marker detection, successfully solving the prognostic stratification dilemma for stage III CRC patients receiving FOLFOX chemotherapy. The study clearly confirmed that traditional single FOXP3 marker cannot accurately define the functional phenotype of regulatory T cells, while the CD3+/CD4+/FOXP3+/PD1− specific subtype of regulatory T cells is an independent favorable prognostic marker for stage III CRC chemotherapy patients. Their high infiltration status can significantly improve patient chemotherapy benefits and prolong survival, while PD1-positive regulatory T cells have no prognostic predictive value. This finding perfectly explains the conclusion controversy in previous related studies and fills the research gap in functional typing of CRC T cell subsets. At the same time, the study verified the clinical practicality of Cell DIVE multiplex imaging technology combined with machine learning algorithms. This technology can achieve standardized and precise quantitative assessment of the tumor immune microenvironment, effectively avoiding subjective errors in manual detection and interference from tumor heterogeneity. However, this study still has certain limitations: it only focused on the FOLFOX chemotherapy population, did not include patients receiving other chemotherapy regimens, and was mainly based on tissue microarray samples. In the future, the sample size can be expanded, the research population can be broadened, and whole tissue section detection can be combined to further verify the generalizability of this immune marker. Overall, the multi-marker T cell typing system constructed in this study provides a new clinical tool for chemotherapy benefit screening and precise prognostic assessment of stage III CRC patients, and also provides new ideas and directions for the research of individualized immunotherapy combined with chemotherapy in CRC.
References
Stachtea X, Loughrey MB, Salvucci M, Lindner AU, Cho S, McDonough E, Sood A, Graf J, Santamaria-Pang A, Corwin A, Laurent-Puig P, Dasgupta S, Shia J, Owens JR, Abate S, Van Schaeybroeck S, Lawler M, Prehn JHM, Ginty F, Longley DB. Stratification of chemotherapy-treated stage III colorectal cancer patients using multiplexed imaging and single-cell analysis of T-cell populations. Mod Pathol. 2022 Apr;35(4):564-576. doi: 10.1038/s41379-021-00953-0. Epub 2021 Nov 3. PMID: 34732839; PMCID: PMC8964416.
EnkiLife mIHC TSA Kits
Product | Catalog Number |
|---|---|
TSA Six-Label Seven-Color Multiplex Immunohistochemistry Kit | |
TSA Five-Label Six-Color Multiplex Immunohistochemistry Kit | |
TSA Four-Label Five-Color Multiplex Immunohistochemistry Kit | |
TSA Three-Label Four-Color Multiplex Immunohistochemistry Kit | |
TSA Two-Label Three-Color Multiplex Immunohistochemistry Kit |